Basic Questions
Germicidal UV (GUV) refers to using ultraviolet radiant energy to inactivate bacteria, mold spores, fungi or viruses. When the process is applied in a given location, it has generally been referred to as ultraviolet germicidal irradiation (UVGI). Because of the public’s concern about ionizing radiation (e.g., X-rays and gamma rays), the term GUV avoids needless concerns about a link with that type of radiation. Another non-technical term is germicidal light, although “light” is technically only visible radiation.
No. Germicidal ultraviolet (GUV) – refers to short-wavelength ultraviolet “light” (radiant energy) that has been shown to kill bacteria and spores and to inactivate viruses. Wavelengths in the photobiological ultraviolet spectral band known as the “UV-C,” from 200 to 280 nanometers (nm), have been shown to be the most effective for disinfection, although longer, less energetic UV can also disinfect if applied in much greater doses. UV-C wavelengths comprise photons (particles of light) that are the most energetic in the optical spectrum (comprising UV, visible, and infrared) and therefore are the most photochemically active.
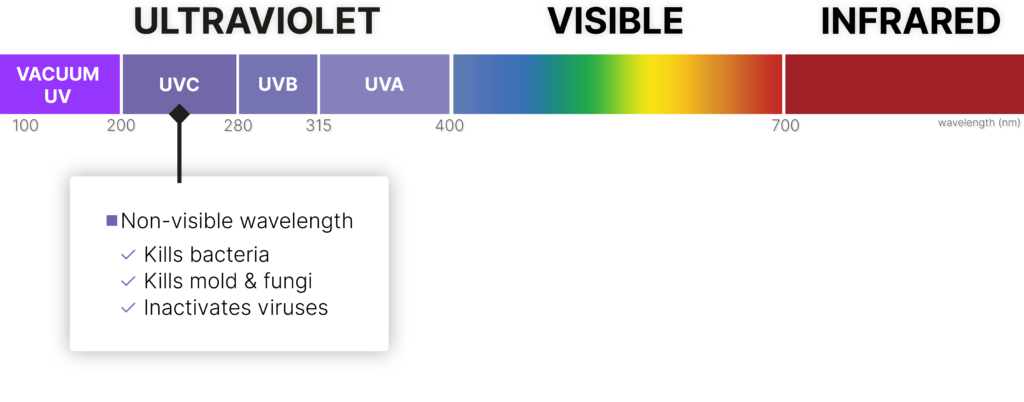
Yes, UV-C kills living bacteria, but viruses are technically not living organisms; thus, we should correctly say “inactivate viruses.” Individual, energetic UV-C photons photochemically interact with the RNA and DNA molecules in a virus or bacterium to render these microbes non-infectious. This all happens on the microscopic level. Viruses are less than one micrometer (µm, one-millionth of a meter) in size, and bacteria are typically 0.5 to 5 µm.
Yes, if the virus is directly illuminated by UV-C at the effective dose level. UV-C can play an effective role with other methods of disinfection, but it is essential that individuals be protected to prevent UV hazards to the eyes and skin. UV-C should not be used to disinfect the hands!
Yes, particularly in the late spring and early summer when the sun is high in the sky and the UV index is high. At a UV Index of 10, the duration to achieve at least a three-log kill of bacteria (99.9% killed) is estimated as less than one hour.[1]
[1] Lytle CD, Sagripanti J-L. Predicted inactivation of viruses of relevance to biodefense by solar radiation. J Virol. 2005;79(22):14244-52.
Medical & Healthcare Questions
The official position of the World Health Organization (WHO) is that this virus is spread by contact with large respiratory droplets, directly or indirectly by touching contaminated surfaces and then touching the eyes, nose, or mouth. However, research is underway to determine the degree of airborne spread—meaning virus in particles so small that they remain suspended in air. Such aerosol results from the evaporation of larger respiratory particles generated by coughs, sneezes, ordinary speech, singing, and possibly by faulty plumbing systems, as occurred with the severe acute respiratory syndrome (SARS) virus. How much of the virus responsible for COVID-19 is spread by the airborne route is not clear, but recommendations for healthcare workers to use fitted respirators, not surgical masks, reveal official concern for airborne transmission. The possibility that inhaled virus may result in more-severe lung damage than acquisition by other routes—for example, via the mouth, nose, or eye—is currently being investigated.
This is important, but difficult to answer in a simple fashion and it depends on how the microbes were made airborne, e.g., from a sneeze or cough, or by being blown up from surfaces or dusted off clothes. The smallest particles (1- to 5-µm droplet nuclei) can remain airborne much longer than cough droplets—for many minutes or even hours.
Commonly used GUV lamps generate predominantly 254-nm UV radiant energy, which is close to the peak germicidal wavelengths of 265 to 270 nm – both in the UV-C range, compared to the longer-wavelength ultraviolet (UV-A and UV-B) in sunlight. GUV radiant energy damages nucleic acids (DNA and RNA), thus preventing replication and leading to the death of virtually all bacteria and inactivation of all viruses—both DNA and RNA types. Bacteria and viruses vary somewhat in UV susceptibility, with environmental organisms, fungal spores, and mycobacteria being relatively harder to kill than more rapidly replicating and non-environmental microbes and most bacteria. But even fungi are effectively killed with high-dose UV, which is used, for example, to treat fungal contamination of air conditioning systems. GUV can be most effectively used to disinfect air in the upper room where ceiling height permits, but can also be used in ventilation ducts and room air cleaners, as noted. As explained below, upper-room UVC is considered the most effective application for room air disinfection, where feasible.
Yes. Some hospitals have used portable GUV fixtures to disinfect air and surfaces in unoccupied, locked rooms as a supplemental control measure to reduce the spread of healthcare associated infections.[2] However, well controlled studies of efficacy are very difficult to conduct and therefore lacking. Medical treatment facilities are using GUV in three primary ways: 1) upper-room UVC fixtures with air mixing, for controlling airborne pathogens in an occupied space; 2) mobile GUV units, to disinfect high-touch surfaces; and 3) GUV in HVAC air handling units, to treat recirculated air and to reduce mold growth on cooling coils. Autonomous (“robot”) systems have been used in some U.S. hospitals and were used in the People’s Republic of China in response to COVID-19.[3] In fighting a war, which this is seen to be, a single weapon is never used; rather, multiple weapons in the armamentarium are exploited.[4] There is no reason not to make full use of GUV with appropriate precautions in this “war” against COVID-19.
[2] Wight W. Germ-killing robots fight drug-resistant pathogens at Army hospitals. 65th Medical Brigade Public Affairs Office. 24 Jul 2017. Online: https://www.army.mil/article/191241/germ_killing_robots_fight_drug_resistant_pathogens_at_army_hospitals. (Accessed 2020 Mar 16).
[3] Ackerman, E. Autonomous robots are helping kill coronavirus in hospital. IEEE Spectrum. 11 Mar 2020. Online: https://spectrum.ieee.org/automaton/robotics/medical-robots/autonomous-robots-are-helping-kill-coronavirus-in-hospitals. (Accessed 2020 Mar 16).
[4] Lee T, Jordan NN, Sanchez JL, Gaydos JC. Selected nonvaccine interventions to prevent infectious acute respiratory disease. Am J Prev Med. 2005;28(3):305-16.
While UV-C could be a secondary infection control measure for disinfecting potential germ-carrying deposits on accessible (not-shadowed) surfaces, its great value would be in disinfecting air in areas where this may be a concern (e.g., intensive care wards, hospital intake facilities [or tents]). Upper-air GUV is the safest, most effective application of UV-C. In special locations, where viral transmission is highly likely, whole-room UVGI (from suspended fixtures directing UV-C downward) could be applied, provided strict precautions can be followed. It is critical that any persons remaining in the space being treated from overhead and side UV-C lamps wear protective clothing and eye protection, or exposure to harmful UV will occur. Whole-room GUV has been safely applied in unoccupied rooms where entry is forbidden during the UVGI.
In the U.S., the Centers for Disease Control and Prevention (CDC) has provided guidelines for the use of UVGI lamps in upper rooms and air handling units (AHUs) as a supplemental control measure for air disinfection.[5, 6, 7]
[5] Sehulster L, Chinn RYW. Guidelines for environmental infection control in healthcare facilities – Recommendations of the Centers for Disease Control and the Healthcare Infection Control Practices Advisory Committee (HICPAC). 2003;52(RR10):1-42.
[6] Jensen PA, Lambert LA, Lademarco MF, Ridzon R. 2005. Guidelines for preventing the transmission of Mycobacterium tuberculosis in health-care settings, 2005. Morbid Mortal Weekly Rep. 2005;54(RR17):1-141.
[7] Centers for Disease Control and Prevention; and National Institute for Occupational Safety and Health. Environmental Control for Tuberculosis: Basic Upper-Room Ultraviolet Germicidal Irradiation Guidelines for Healthcare Settings. Washington, DC: Department of Health and Human Services; 2009.
The most fundamental concept in photobiology is the action spectrum (or relative response) for a given effect. Although there is a standardized germicidal action spectrum in the IES Handbook,[8] it was based on inactivation of E. coli bacteria, and action spectra for spores, other bacteria, and different viruses can vary. This standardized action spectrum extends from 235 nm to 313 nm and peaks at approximately 265 nm. A wavelength of 254 nm has a relative efficacy of 0.85; by contrast, 313 nm in the UV-B has a relative efficacy of only 0.01.
Germicidal effectiveness is proportional to the exposure dose (radiant exposure, typically in millijoules* per square centimeter, mJ/cm2, or joules per square meter, J/m2), which is the product of the dose-rate (irradiance, typically in mW/cm2 or W/m2) and time (from 1 μs to several hours). A nonlinear relationship exists between UV exposure and germicidal efficacy. For example, if a certain UV exposure kills 90% of a bacterial population (frequently referred to as “one-log kill”), doubling the exposure time or intensity can kill only 90% of the residual 10%, for an overall germicidal efficacy of 99% (“two-log kill”). Likewise, a 50% decrease in dose or exposure time decreases efficacy only from 99% to 90%.
Humidity can reduce the effectiveness of germicidal UV radiation. There is a reference dose to attain a survival of 37%; however, in practice a GUV dose of interest is 3 or 4 log-kills, corresponding to 99.9% or 99.99% inactivation, respectively. To be effective in practice, achieving two log-kills (99% inactivation) is frequently accepted.
[8] DiLaura D, Houser K, Mistrick R, Steffy S (editors). The Lighting Handbook, 10th ed. New York: Illuminating Engineering Society; 2011.
* One joule is equal to one watt times one second. (Or, 1 W = 1 J/s) A millijoule is one-thousandth of a joule.
Treating Room Air with UVC
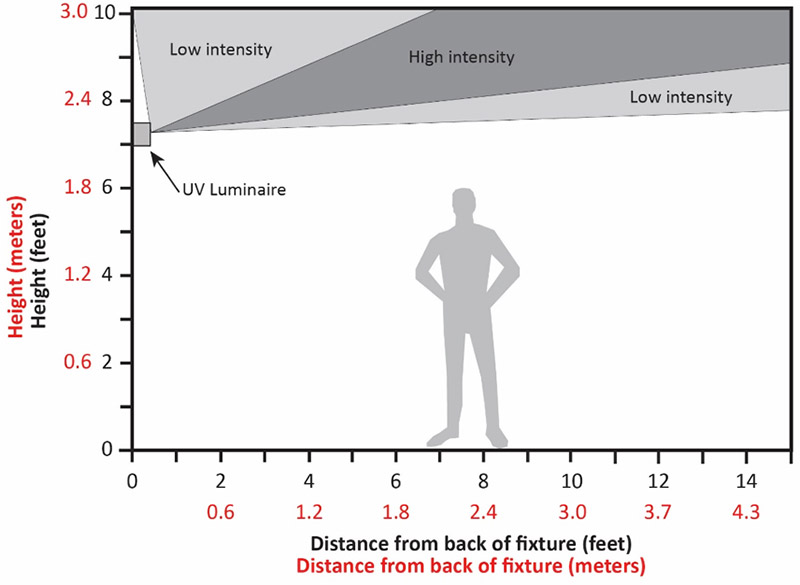
upper-room UVC is a safe means of air disinfection that is possible in rooms with high ceilings. In this method, specially designed and installed UV-C fixtures that irradiate only the air above 2.1 meters (7 feet) constantly disinfect the upper air volume. This is most effective when there is constantly mixed air by fans and HVAC ventilation, but even without strong ventilation or fans, air constantly mixes by movements and normal convective currents.
upper-room UVC disinfects large volumes of room air (above occupants’ heads) at once, resulting in high “equivalent” air changes per hour (ACH) in terms of air disinfection only—GUV does not dilute odors or CO2, the main functions of building ventilation. Odor control and CO2 removal are accomplished by relatively low levels of ventilation (1 to 2 ACH), but air disinfection requires much higher rates of ventilation (6 to 12 ACH), or the equivalent produced by upper-room UVC. Two hospital controlled studies [9, 10] have shown upper-room UVC to be about 80% effective against tuberculosis (TB) spread. Even when GUV is confined to the upper room, good air mixing (ideally with low-velocity ceiling fans but easily accomplished by other types of forced-air ventilation) results in very high equivalent ACH in the lower, occupied space—estimated to be an additional 24 ACH in a South African study.[9]
When UV is used in ducts, although it ensures that recirculated air does not have viable pathogens, it unfortunately does relatively little to prevent person-to-person transmission in a room where both an infectious source and other susceptible persons share the same air. For effective interruption of transmission, air disinfection has to occur in the same room where transmission is occurring. Portable air cleaners can be placed in rooms where there is a risk of transmission, but moving large volumes of air through any device is difficult, limited by the clean-air delivery rate of the portable air cleaner. Often when the clean air delivery rate is converted to equivalent ACH, the result is a disappointing 1 to 2 ACH, far too little to effectively prevent transmission. A large air cleaner in a small room may be effective, but for larger rooms, air cleaners are simply an impractical approach to high levels of air disinfection, compared to upper-room UVC. Air cleaners may have value in a confined space where GUV is desired.
GUV Safety
UVGI lamp emissions can pose a workplace safety and health hazard to the eyes and skin if the lamps are improperly used or installed. However, these lamps can be used safely if workers are informed regarding the hazards and follow appropriate precautions. upper-room UVC has been safely used for preventing airborne transmission for at least 70 years. A great deal is known about the human exposure limits of 254-nm UV (UV-C) irradiation. Compared to the UV-A and UV-B in sunlight, UV-C is almost entirely absorbed by the outer dead layer (stratum corneum) and outer skin (outer epidermis), with very limited penetration to the deeper cellular layers of skin where new cells are constantly created. For comparison, the current daily safety limit of 254-nm UV-C for 8 hours is 6.0 mJ/cm2, whereas less than ten minutes of summer sun exposure at a UV Index of 10 can deliver the equivalent limiting daily safety dose[11] because of its much more-penetrating UV-A and UV-B. A study of continuous monitoring of healthcare workers and patients in an upper-air GUV installation recorded no more than 1/3 of the 8-hour dose. Because it has no outer dead protective layer, the human eye is the organ most susceptible to sunlight and upper-room UVC. Exceeding the threshold level value (TLV) in the lower room will result in painful irritation of the cornea similar to overexposure on a sunny day, especially from sun reflected from water or snow. The damage is painful but transitory, with corneal shedding and replacement in a day or two. When the UV-C source is overhead, the eyes receive very little exposure during normal activities; this is demonstrated in sunlight when the sun is overhead—there is hazardous exposure of the skin but not the eyes. There are no known long-term consequences from an accidental UV-C overexposure.[12] Most eye injuries result from workers on ladders cleaning fixtures or working in the upper room without first turning off the fixtures.[13] For this reason, only trained maintenance workers should be working in the upper room or replacing in-duct lamps. Eye injuries have resulted from insufficient training or improper installation—e.g., workers mistakenly installing an upper-room UVGI fixture upside-down after bulb replacement.[14]
[11] American Conference of Governmental Industrial Hygienists. 2020 Threshold Limit Values and Biological Exposure Indices. Cincinnati: ACGIH; 2020.
[12] International Commission on Illumination (CIE). CIE 187:2010, UV-C Photocarcinogenesis Risks from Germicidal Lamps. Vienna: CIE; 2010.
[13] Sliney D. Balancing the risk of eye irritation from UV-C with infection from bioaerosols. Photochem Photobiol. 2013;89(4):770-6. [Erratum in: Photochem Photobiol. 2013 Jul-Aug; 89(4):770].
[14] Sensakovic JW, Smith LG. Nosocomial ultraviolet keratoconjunctivitis. Infect Control. 1982;3:475-6.
UV-C penetrates only the superficial layers of the skin and eye, with the shortest wavelengths hardly penetrating at all to living cells (epidermis), so only a very mild, transitory “sunburn” (erythema) occurs from accidental over-exposure of skin areas. Even though GUV lamps can pose a theoretical delayed hazard, incidental UV exposures in the workplace would not significantly increase one’s lifetime risk for cataract or skin cancer when compared to daily exposure to the UV radiant energy in sunlight. Solar UV is much more penetrating and reaches the germinative (new-cell producing) layers in the skin, with the result that skin cancer risk is significant, and sunburns can be severe. There is a small amount of UV-B (297, 303, 313 nm) from a low-pressure mercury lamp, but this is insignificant unless exposures are experienced at least an order of magnitude or more above the safety limits for 254 nm.[15]
[15] International Commission on Illumination (CIE). CIE 187:2010, UV-C Photocarcinogenesis Risks from Germicidal Lamps. Vienna: CIE; 2010.
GUV Applications
There are very sophisticated programs to calculate the lamp sizes and in-air dose requirements in terms of energy required for space and radiant fluence (joules per square meter, J/m2) across a cross-section of a UV-C beam, but there is a much simpler evidence-based dose that has been developed over many years for TB control, typically specified as about 17 mW of 254-nm lamp-emission radiant power per cubic meter (m3) of space to disinfect air.[16] Although this sounds too simplistic to be true, since air in any room is always moving and mixing, one can correctly assume that all air will be treated—the better the air mixing, the sooner this will happen. Studies at the Harvard School of Public Health[16, 17] and elsewhere show log units of reduction equivalent to 24 ACH to achieve 80% reduction of transmission. Of course, 100% reduction is not possible, because of the multiple modes of transmission. To disinfect surfaces, this depends on the type of surface and its cleanliness; recommended exposures vary from 200 to 1,000 J/m2 (20 to 100 mJ/cm2).[18]
[16] Mphaphlele M, Dharmadhikari AS, Jensen PA, Rudnick SN, van Reenen TH, Pagano MA, Leuschner W, Sears TA, Milonova SP, van der Walt M, et al. Institutional tuberculosis transmission. Controlled trial of upper room ultraviolet air disinfection: A basis for new dosing guidelines. Amer J Respir Crit Care Med. 2015;192(4):477-84.
[17] Miller SL. Upper room germicidal ultraviolet systems for air disinfection are ready for wide implementation (editorial). Am J Respir Crit Care Med. 2015;192(4):407-9.
[18] Jelden KC, Gibbs SG, Smith PW, Schwedhelm MM, Iwen PC, Beam EL, Hayes AK, Mar4on N, Kratochvil CJ, Boulter KC, et al. Nebraska Biocontainment Unit patient discharge and environmental decontamination after Ebola care. Amer J Infect Control. 2015;43(3):203-5.
There are a number of dedicated meters available; however, a wide range of scale is normally required, e.g., a range from 0.1 to 100 microwatts per square centimeter (µW·cm-2).[19] Safety readings require the lower range, and efficacy requires a range up to at least 10 mW·cm-2. A common practice is to have two calibrated meters: one in reserve and for reference. The two instruments should be periodically compared. The user should retain the manufacturer’s instructions, including a description of the meter, its safe use, and maintenance and calibration of it. Some healthcare facilities contract with a full, outside maintenance contractor that uses calibrated meters and correctly and safely replaces burned-out lamps. Some users retain a simple, less precise meter for staff to use, but the installer uses a professional meter.[20]
[19] Reed NG, Wengraitis S, Sliney DH. Intercomparison of instruments used for safety and performance measurements of ultraviolet germicidal irradiation lamps. J Occup Environ Hyg. 2009;6(5):289-97.
[20] End TB Transmission Initiative. Maintenance of Upper-Room Germicidal Ultraviolet (GUV) Air Disinfection Systems for TB Emission Control. Copenhagen: United Nations Office for Project Services (UNOPS); 2020. Available online: http://www.stoptb.org/wg/ett/. (Accessed 2020 Apr 12).